RESEARCH ARTICLE
- Aamir Jalal Al Mosaw 1
The National Training and Development Center and Baghdad Medical City, Iraq.
*Corresponding Author: Aamir Jalal Al Mosaw
Citation: Aamir Jalal Al Mosaw (2024), William Mackenzie Blighted ovum syndrome: An educational ultrasound image and review, Community and Public Wellness Nursing (CPWN) 1(1), DOI: 10.1875/cpwn.2024/001
Copyright: © 2024, Aamir Jalal Al Mosaw, this is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: January 05, 2024 | Accepted: February 09, 2024 | Published: February 13, 2024
Abstract
Background: A blighted ovum syndrome occurs when a pregnant female had anembryonic gestation with normal gestational sac, but without an embryo. The embryo may have not developed or it developed, but has reabsorbed. William Mackenzie was most probably the first to provide a detailed account of the condition which included a description of a blighted ovum dissection. Since the 1970s, blighted ovum syndrome has been increasingly recognized as a cause of recurrent miscarriages. The aim of this paper is to provide and educational ultrasound image and an educational review.
Patients and methods: The case of a 39-year-old female who experienced a blighted ovum syndrome is described.
Results: A 39-year-old primigravida female was tested positive for pregnancy, and within few days she experienced spotting of blood. Ultrasound examination showed anteverted gravid uterus with a single gestational with yolk sac without fetal pole. The mean gestational sac diameter was at six weeks. Both adnexa were normal and the cervix was closed. Four days later the patient experienced pain and bleeding indicating miscarriage.
Conclusion: This paper emphasizes the vital role of ultrasound examination in the timely and confident diagnosis of blighted ovum syndrome.
Keywords: Ultrasound examination, blighted ovum syndrome.
Introduction
A blighted ovum syndrome occurs when a pregnant female had anembryonic gestation with normal gestational sac, but without an embryo. The embryo may have not developed or it developed, but has reabsorbed. William Mackenzie (Figure-1) was most probably the first to provide a detailed account of the condition which included a description of a blighted ovum dissection [1, 2]. Since the 1970s, blighted ovum syndrome has been increasingly recognized as a cause of recurrent miscarriages [3]. The aim of this paper is to provide and educational ultrasound image and an educational review.

Patients and methods
The case of a 39-year-old female who experienced a blighted ovum syndrome is described.
Results
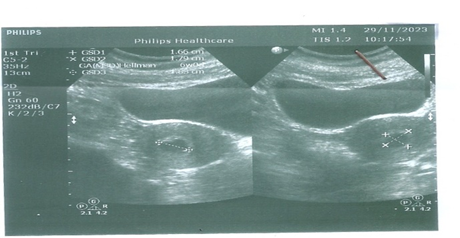
A 39-year-old primigravida female was tested positive for pregnancy, and within few days she experienced spotting of blood. Ultrasound examination (Figure-2) showed anteverted gravid uterus with a single gestational with yolk sac without fetal pole. The mean gestational sac diameter was at six weeks. Both adnexa were normal and the cervix was closed. Four days later the patient experienced pain and bleeding indicating miscarriage
Discussion
The diagnosis of blighted ovum syndrome by ultrasound examination has been reported as early as the 1972. Normally, an embryo can be seen on an ultrasound six weeks after the last menstrual period. In blighted ovum syndrome, an early death of the embryo occurs with continued formation of the trophoblast. Therefore, there will be generally a yolk sac that can be seen on ultrasound, but without a fetal pole.
The ultrasound diagnosis of blighted ovum syndrome is based on finding a gestational sac diameter more than 25 mm with no yolk sac, or a gestational sac diameter more than 25 mm without embryo [4, 5].
In 1979, Schweditsch et al reported the hormonal profiles of six females who experienced blighted ovum syndrome, and terminated in miscarriages. Serum chorionic gonadotropin levels were lower than normal or at the lowest normal level in five of six females. Three females had progesterone levels within 1 SD of the normal, with normal level of serum estradiol. Schweditsch et al suggested that early pregnancy is characterized by increasing serum chorionic gonadotropin and estradiol levels and lowering of serum progesterone level from the 5th to the 8th week of gestation. They emphasized that subnormal level of serum estradiol should raise the suspicion of a blighted ovum syndrome [6].
Conclusion
This paper emphasizes the vital role of ultrasound examination in the timely and confident diagnosis of blighted ovum syndrome.
References
-
Mackenzie W. Dissection of a Blighted Ovum, with Remarks. Edinb Med Surg J 1836 Jan 1; 45(126):39-48.
Publisher | Google Scholor -
Cromwell BM. A Case of Double Pregnancy:-One Ovum Being Blighted and Discharged as a Mole; the Other Expelled Two Weeks Afterwards. Atlanta Med Surg J 1867 Aug; 8(6):249-252.
Publisher | Google Scholor -
Poland BJ. Embryonic development in patients with recurrent abortions. Fertil Steril 1971 May; 22(5):325-31.
Publisher | Google Scholor -
Donald I, Morley P, Barnett E. The diagnosis of blighted ovum by sonar. J Obstet Gynaecol Br Commonw 1972 Apr; 79(4):304-10.Doi:10.1111/j.1471-0528.1972. tb158 01.x.
Publisher | Google Scholor -
Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy; Barnhart KT, Benacerraf BR, Brown DL, Filly RA, Fox JC, Goldstein SR, Kendall JL, Lyons EA, Porter MB, Pretorius DH, Timor-Tritsch IE. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013 Oct 10; 369(15):1443-51. Doi: 10.1056/NEJMra1302417.
Publisher | Google Scholor -
Schweditsch MO, Dubin NH, Jones GS, Wentz AC. Hormonal considerations in early normal pregnancy and blighted ovum syndrome. Fertil Steril 1979 Mar; 31(3):252-7.Doi: 10.1016/s0015-0282(16)43870-7.
Publisher | Google Scholor