RESEARCH ARTICLE
1Department of Midwifery, Aksum, Aksum University
2Department of Midwifery, Mekelle, Mekelle University
2Department of Midwifery, Mekelle, Mekelle University
1Department of Midwifery Aksum, Aksum University
*Corresponding Author: SUrafal aregawi
Citation: SUrafal aregawi , Magnitude and Factors Associated with Postnatal Cord Care Practice among Mothers in Mekelle City, Tigray, Ethiopia, 2019 GC: A Community Based Cross sectional Study, Clinical Cardiology and Cardiovascular Procedures, vol 1(1). DOI: https://doi.org/10.64347/3066-2656/CCCP.003
Copyright: © 2024, SUrafal aregawi Vitus, this is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: November 01, 2024 | Accepted: November 05, 2024 | Published: November 22, 2024
Abstract
Background: Cord care is one component of essential newborn care which comprises a sequence of steps. Immediately at birth and during post natal period, umbilical cord care is related with different traditional practices and believes. There is limited evidence regarding umbilical cord care and its associated factors in Ethiopia as well as in the study conducted. The aim of this study was to assess magnitude and factors associated with post natal cord care practice among mothers in Mekelle city, Tigray, Ethiopia, from November to December 2019GC.
Method: A Community based cross-sectional study was conducted from November 2019 up to December 2019 among 592 postnatal mothers in Mekelle city, Tigray Ethiopia. Multi-stage approach to sampling was used to select the kebeles, then systematic sampling was used, to select the participants. Data were collected by structured and pre-tested interviewer administered questionnaire; the collected data was entered into Epi-Data 4.2 then exported and analyzed using Statistical package for social sciences (SPSS) version 20. Results of the study participants were described and presented by using frequencies, percentages, summary measures, tables and graphs. Bivariate and multivariable logistic regressions were used to identify factors associated with postnatal cord care practice by using 95% confidence interval.
Results: Most of 565 (95.3%) respondents were married and around 111(18.8%) respondents were unable to write and read. From the total respondents, 385(65%) mothers were multipara and almost all 589(99.5%) mothers gave birth at health institution. proportion of mothers who practiced good postnatal cord care was found to be 75.7% & Butter was the commonly applied substance to cord stump, with duration ranging from one to eighteen days. mothers who’s their baby’s faced problem of umbilical cord stumps were 39(6.6%). Age of the mother, educational level, knowledge of the mother on cord care, source of information about cord care and ever counseled about cord care were significantly associated with postnatal cord care practice.
Conclusions: Even though the prevalence of good cord care practice is high, there is still a use of potentially harmful substances and still many neonates are at risk of developing Omphalitis and neonatal sepsis.
Keywords: Cord Care, Postnatal Mothers, Community
Introduction
Umbilical cord care during the postnatal period includes, washing hands with clean water and soap before and after care, keeping the cord stump dry & exposed to air or loosely covered with clean clothes, If soiled, the cord should be washed with clean water and soap and dried with clean towel. The diaper should also be put slightly below the umbilicus. (3)
Based on different studies, immediately at birth and during post natal period, Umbilical cord care is linked with different traditional practices and believes, and substances are applied to cord stump like: ash, butter, fresh colostrum. Those substances are contaminated with different pathogens and increase the risk of infection. (4 & 5)
The World health organizations WHO guide line endorse clean and dry cord care (no application of any substances). But, in areas where hygienic practices are poor antiseptics is promoted for cleaning the cord, (7.1% chlorhexidinedigluconate aqueous solution or gel, delivering 4% chlorhexidine) povidine iodine, gentian violet. (7)
Annually more than half a million neonatal mortality is occurred due to bacterial infections, Umbilical cord infection was a significant contributor of those deaths. This is due to the fact that umbilical cord wound is a potential source of entry of infectious pathogenic microorganisms. In 2006 at University of Cocody Teaching Hospital (CHU) in Ivory-Coast, 69.3% of bacterial infections are related with traditional care. Of these, two third originated from the umbilicus(13).
In Ethiopia where neonatal mortality is high, more than 18% percent of neonatal death is due to neonatal sepsis. The main contributor of neonatal sepsis is umbilical cord infection (omphalitis).(8) Ethiopia’s national health strategy has planned on reducing neonatal death, from 28/1000live births to 11/1000livebirths by 2020 (18).
The federal ministry of health of Ethiopia on newborn umbilical cord care during postnatal period recommends keeping the cord clean and dry, with no application of any substance, (dry cord care ) (8).
There is little information regarding cord care during post natal period. So this study will help to address harm full practices related with umbilical cord care during post natal period
Methods
Study area and period
This study was conducted in Mekelle city. Mekelle is the capital city of Tigray National Regional State and is located in the Northern part, at 783 km from, Addis Ababa, the capital city of Ethiopia .The city administratively divided into seven sub cities and are subdivided to 33 Kebelles. Based on Central Statistical Agency of Ethiopia, 2015, the total population of the city is 480,217.There are one comprehensive specialized hospital, two general hospital, one primary hospital and seven health centers. There are four General hospitals, thirty eight clinics owned by private organizations. From November 2018 to March, 2019 GC
Study design
Community based cross sectional study design was conducted.
Source population
All postnatal mothers in Mekelle city
Study population
Mothers who gave birth in the last six months prior to data collection in the selected kebeles
Eligibility criteria
Inclusion criteria
Mothers who have a baby from birth up to six months prior to study period
Mothers who are permanent resident of Mekelle city
Exclusion criteria
Mothers with mental health problem or that have communication difficulty to get the necessary data.
Sample size Determination and sampling procedures
The required sample size was determined using formula for single population proportion (n = (Z/2)2pq/d2)) and on the following assumption
n = 
Where:
n= is the desired sample (when population is>10,000)
Z= is the standard normal deviation usually set at 1.96
p = is the the level of good cord care practice which was conducted in Ugandain January 2018 was 38%.(27)
q = 1-p = 1- 0.38 = 0.62
d = the degree of accuracy desired usually set at 0.05.
Therefore n =  =
=  = 362, using design effect multiplied by1.5, n=543
= 362, using design effect multiplied by1.5, n=543
Therefore n=543 with contingency 10%, the final sample size was 596
Sampling procedure
Mekelle city has seven sub cities and 33 kebeles. A multistage approach to sampling was used to select kebeles; hadnet,ayder and semyensub cities were selected by simple randomsampling. Three kebeles from each selected sub cities have been selected again by simple random sampling, and then systematic random sampling was used to select the participants. The total sample size was proportionally allocated to each selected sub cities and kebeles by their average number of deliveries for the last six months.
Preliminary survey was conducted with the help of health extension workers to identify households with a postnatal mother less than six months at each selected kebeles. K value was calculated for each kebeles. Then actual respondents were selected at regular interval (every k) by systematic random sampling.
K=N/n, K approximately= 2
Variables of the study
Dependent variable
Postnatal Cord care practice
Independent variables
Socio Demographic factors: Age, Occupation, Residence, Level of income, Educational status, Marital status and Distance to health institution
Health service exposure: Post natal follow up(PNC), Place of delivery, ANC, Parity and Counseling during peri-natal follow up
Source of information: Health care worker, Non health care worker(mother, neighbor) and Media
Knowledge and attitude of mothers on newborn cord care
Operational definitions
Good Postnatal Cord Care; if the mother does not put any substance to the cord stump of her baby or if she keeps dry
Poor Postnatal Cord Care; if the mothers put any substance to the cord stump of her baby or if she doesn’t keep it dry(11)
Good knowledge of cord care; scores above the 50th percentile was adjudged good knowledge
Poor knowledge of cord care; scores below the 50th percentile was adjudged poor knowledge.(1)
Knowledge: Ability to describe the procedure of umbilical cord care
Practice: It refers to the activities which are undertaken in relation to the umbilical cord care
Results
Socio-economic and demographic characteristics
A total of 596 mothers of babies aged up to 6 months were included in the study with a response rate of 592(99.4%). The mean age of the mothers was 28.61 years with a standard deviation of±4.219 years. Most of 565 (95.3%) the respondents were married and around 111(18.8%) respondents are unable to write and read. Majority, 558 (94.3%) of mothers were orthodox in religion (Table 1).
Table 1: Socio-demographic Characteristics of mothers who gave birth in the last six months in Mekelle city Tigray Ethiopia, February 2019 (n=592).
| frequency | Percentage | ||
Marital statues (n= 592) | Single | 19 | 3.2 |
| Married | 564 | 95.3 | |
| Divorced | 9 | 1.5 | |
Educational Level of Mother (N=592) | un able to write and read | 111 | 18.8 |
| Primary | 137 | 23.2 | |
| Secondary | 125 | 21.2 | |
| diploma and above | 218 | 36.9 | |
| husband educational level(n=564) | un able to read and write | 62 | 10.6 |
| Primary | 202 | 34.4 | |
| Secondary | 195 | 33.2 | |
| diploma and above | 128 | 21.8 | |
Occupation (n=592) | Governmental | 102 | 17.2 |
| Merchant | 149 | 25.2 | |
| Private employee | 72 | 12.2 | |
| house wife | 269 | 45.4 | |
husband occupation (n=564) | Gove mental employee | 133 | 23.5 |
| Merchant | 281 | 49.7 | |
| Private | 111 | 19.6 | |
| Farmer | 3 | 0.5 | |
| no work | 37 | 6.5 | |
Religion (592) | Orthodox | 558 | 94.3 |
| Muslim | 33 | 5.6 | |
| Protestant | 1 | 0.2 | |
Ethnicity (n=592) | Tigray | 578 | 97.6 |
| Afar | 2 | 0.3 | |
| Amhara | 12 | 2.0 | |
Income (n=592) | 1400 and less | 25 | 4.2 |
| 1401 up to 2350 | 20 | 3.4 | |
| 2351 up to 3550 | 95 | 16.0 | |
| 3551 up to 5000 | 136 | 23.0 | |
| above 5000 | 316 | 53.4 | |
| age (n=59) | 30 and below | 449 | 75.8 |
| 31 and above | 143 | 24.2 | |
Knowledge of mothers on cord care
The proportion of mothers who have good knowledge on cord care practice was 63.5%. Among the total respondents, 386(65.2%) had information about cord care at least one. From these who have information about cord care, 295(76.4%) had obtained from health care worker.
Maternal health service utilization and obstetric conditions
From the total respondents, 385(65%) were multi-para and 30(5.1%) grand mult-ipara. Majority of the participants 458(77.4%) had 4 and above antenatal care. Regarding place of delivery almost all 589(99.5%) mothers gave birth at health institution. Mothers who have first, second, third and fourth postnatal visit was found to be; 590(99.7%), 157(26.4%), 41(6.9%), and 35(5.9%) respectively. More than three fourth 452(76.4%) of Mothers were ever counseled during perinatal follow up on how to provide cord care. Of those who were counseled about cord care, 98(18.3%) counseled during antenatal visit.
Table 2: The obstetric and maternal health service exposure characteristics of respondents in the last six months in Mekelle city Tigray, Ethiopia February 2019 (n=592)
| Variable | Frequency | percentage | |
Mode of delivery (n=592) | spontaneous vaginal delivery | 471 | 79.6 |
| instrumental delivery | 28 | 4.7 | |
| cesarean section | 93 | 15.7 | |
| 1st PNC | `no | 2 | 0.3 |
| Yes | 590 | 99.7 | |
2ndPNC
| No | 436 | 73.6 |
| Yes | 156 | 26.4 | |
| 3rdPNC | No | 551 | 93.1 |
| Yes | 41 | 6.9 | |
| 4thPNC | No | 556 | 93.9 |
| Yes | 35 | 5.9 | |
| Parity(n=592) | Primipara | 177 | 29.9 |
| multi para | 385 | 65.0 | |
| grand multi para | 30 | 5.1 | |
| ever counseled about cord care(n=592) | No | 140 | 23.6 |
| Yes | 452 | 76.4 | |
Number of ANC visits (n=592) | one visit | 8 | 1.4 |
| 2-3 visits | 116 | 21.3 | |
| 4 and above visits | 458 | 77.4 | |
Application of substance on cord stump
From the total participants, 144(24.3%) were applied different substances to their babies umbilical cord stump & butter was the commonly applied substance. Figure 1
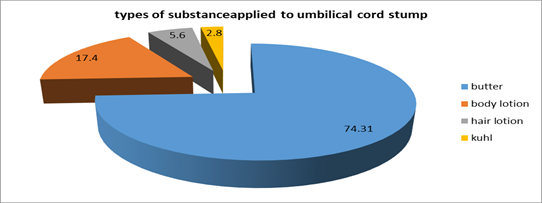

Figure 1: types of substances applied to umbilical cord stump among mothers in the last six months in Mekelle city Tigray Ethiopia February 2019 (n=144)
Figure 2: Purpose of substance application to umbilical cord stump among mothers in the last six months in Mekelle city Tigray Ethiopia February 2019(n=144)
The average time of cord stump separation was 7.33 days, ranging from four up to fifteen days. But twenty seven mothers (4.56%) explained that they don’t remember when the cord stump was separated.
The proportions of mothers who their baby’s faced problem of umbilical cord stumps were 39(6.6%). Out of those baby’s faced with cord problem, the commonly occurred were, swelling of the umbilicus, redness, puss discharge and cord bleeding in 14(35.9%), 11(28.2%), 13(33.3%), and 1(2.6%) respectively.
Factors associated with post natal cord care practice
The odds of good practice in these mother with educational level of diploma and above [AOR=6.290, 95%CI= (1.956, 20.224)] was about 6.29 times of these mother who were un able to read and write. Similarly mothers with a good knowledge about cord care (AOR=7.580, 95%CI= [3.399, 16.904]), were more likely practices a good umbilical cord care than those with poor knowledge (Table 3).
Table 3: Factors associated with postnatal cord care practice among mothers who gave birth in the last six months in Mekelle city, Tigray Ethiopia, February 2019
| good cord care practice | Poor cord care practice | COR (95%CI ) | AOR (95%CI ) | ||
Frequency (%) | Frequency (%) | ||||
| ever counseled about cord care | Yes* | 374(83.3) | 78(54.4) | 4.274(2.83, 26.452) | 8.183(3.442, 19.456) |
| No | 74(16.7) | 66(45.8) | 1 | 1 | |
| knowledge of the respondent | Good* | 229(69) | 16(29.6) | 5.280(2.81,6 9.901) | 7.580 (3.399, 16.904) |
| Poor | 103(31) | 38(70.4) | 1 | 1 | |
| age of the mother | 30 and below* | 373(80.3) | 76(52.8) | 1 | 1 |
| 31 above | 75(16.9) | 68(47.2) | 0.231 (0.153, 0.349) | 0.411(0.181, 0.932) | |
Educational Level of Mother | un able to write and read* | 71(64) | 40(36) | 1 | 1 |
| Primary | 77(56.2) | 60(43.8) | 0.723(0.432, 1.209) | 0.658(0.238, 1.817) | |
| Secondary | 92(73) | 33(27) | 1.571(0.901, 2.737) | 1.115(0.378, 3.292) | |
| diploma and above | 208(95.4) | 10(4.6) | 11.775(5.599, 24.763) | 6.290(1.956,20.224) | |
Family Income | income_cat** | 11(2.5) | 14(9.8) | 1 | 1 |
| income_cat(1) | 14(3.1) | 6(4.2) | 2.970(0.859, 10.265) | 0.457 (0.017. 12.473) | |
| income_cat(2) | 76(17) | 19(13.3) | 5.091(1.996, 12.982) | (0.707 (0.049, 10.228) | |
| income_cat(3) | 90(20.1) | 45(31.5) | 2.545(1.070, 6.057) | (0.607(0.045. 8.106) | |
| income_cat(4) | 257(57.4) | 59(41.3) | 5.544(2.396, 12.827) | 1.699 (0.132.21.796) | |
Occupation of the mother | Governmental* | 72(16.1) | 30(20.8) | 1.052 (0.639, 1.733) | (0.441(0.155, 1.250) |
| Merchant | 126(28.3) | 22(15.3) | 2.531 (1.502, 4.265) | 1.419(0.494, 4.070) | |
| Private employee | 62(13.8) | 11(7.6) | 3.070 (1.457, 6.466) | 8.990(1.534, 52.687) | |
| house wife | 187(41.7) | 82(56.2) |
1 | 1 | |
| Source of information | Health care worker* |
269(91.2) |
26(8.8) | 4.598(2.523, 8.380) | 4.310(2.006, 9.259) |
| non health care worker | 63(29.2) | 28(30.8) |
1 | 1 | |
*=p-value <0 xss=removed xss=removed xss=removed>
Discussion
Although the proportion of mothers who practiced good postnatal cord care is comparatively high, significant numbers of mothers were still applying harm full substances to the cord stump.
The prevalence of good cord care practice in this study (75.7%) were higher than the study done in India30%,by2012(9),in Uganda 38% by 2010(27), Chencha district southern Ethiopia52.9% by 2018,(20) and Mereb-Leke woreda 67.3% by 2016(22). The practice difference could be these studies were conducted at rural setting and the proportion of home delivery is high which may expose mothers to unclean cord care. However it was similar with the study done in Plateau State, Nigeria, 77.8%, by 2018(1).
Diploma and above mothers were more likely practicing good post natal cord care than these mothers with unable to write and read. This is nearly consistent with the study conducted in Bayelsa State Nigeria;(24) the provision of appropriate new born cord care increases with increasing educational level. This might be because education increases the tendency to get service and to read materials related to baby care.
The study revealed that, mothers with good knowledge about cord care were more likely practicing a good postnatal cord care as compared to those mothers with a poor knowledge. This is in line with the cross-sectional study done in Nepal, (23) as well as the study conducted in Nigeria(1).The reason could be those mothers with good knowledge may have more health service utilization behavior and could differentiate the harmful and beneficial activities provided for their baby.
Age was also another factor associated with postnatal cord care practice. Mothers with age of 31 and above practices post natal cord care 58.9% less likely as compared to those with age of 30 and below (AOR=0.411, 95%CI=[0.181, 0.932]).But study conducted in Nigeria shows that; older age mothers practices good cord care than those of younger age mothers(24). The difference could be in the current study younger age mothers are more educated and employed. Older age mothers may be influenced by the traditional care.
The other significant factor associated with post natal cord care practice was Source of information. Mothers whose sources of information about cord care from health care worker more likely practice good postnatal cord care as compared to those their source of information was from non-health care workers. This is consistent with the study conducted in Kenya (11). This similarity might be information obtained from health professional may be the real information and trusted.
This study tried to test new variables, among them mother occupation and counseling about cord car was found to be significantly associated. Private employee mothers (AOR=8.99, 95%CI= [1.534, 52.687]).were more likely to practice a good postnatal cord care as compared to these house wife mothers. The reason could be house wife mothers expends most of their time at home and are less likely to access and exposed to information than employed mothers.
The study revealed that respondents who ever counseled about cord care during their peri-natal follow up (AOR=8.183, 95%CI= [3.442, 19.456]) were practicing good postnatal cord care practice comparing with not ever counseled about cord care. This is due to the fact that counseling about cord care during peri-natal period increases awareness and promotes the like hood of providing good cord care.
Conclusion
Even though the prevalence of good cord care practice is high, there is still a use of potentially harmful substances for cord care and still many neonates are at risk of developing Omphalitis and neonatal sepsis.
Acronyms and abbreviations
ANC: Antenatal Care
AOR: Adjusted Odds Ratio
CSA: Central Statics Agency
COR: Crude odds ratio
EBF: Exclusive Breast Feeding
EDHS: Ethiopian Demographic and Health Survey
ETB: Ethiopian Birr
ENC: Essential Newborn Care
HI: Health Institution
LMICs- Low and Middle Income Countries
MDG: Millennium Development Goal
SPSS: Statistical Package for Social Science
SDG: Sustainable development goals
WHO: World Health Organization
Acknowledgment
We would like to thank Mekelle University, College of Health sciences, Tigray Region Health Bureau, Mekelle city health office, study participants, and data collectors for their contribution in the success of our work
Funding Statement
The research for this project is unfunded. The authors paid for all expenses associated with gathering and analyzing the data.
Data availability
The data sets during and/or analyzed during the current study available from the corresponding author on reasonable request
Authors' contributions
SA: conceived and designed the study, analyzed the data and wrote the manuscript. GK, GA, AB, TA, GG, BH, AG, involved in data analysis, drafting of the manuscript and advising the whole research paper and also were involved in the interpretation of the data and contributed to manuscript preparation. Similarly, all authors have read and approved the final version of the manuscript.
Ethical approval and consent to participate
Ethical clearance was obtained from the ethical review board of Mekelle University College of health science to Mekelle city administration health office, then to each elected sub-cities; Informed, written and signed consent was obtained from each health office coordinator of the sub-cities. Informed consent was obtained from each participant after explaining the purpose and benefits of the study. Participants were informed about the minimal risk that it had taking part in the study, their volunteerism and the right to leave the interview at any time they want. Confidentiality of the study participants’ information was also ensured by coding the questionnaire.
Competing Interests
The author(s) of this manuscript have not disclosed any financial conflicts of interest with this work, nor have they indicated any non-financial conflicts of interest with this work, such as political, personal, religious, ideological, academic, commercial, or any other conflicts.
Conclusion
Even though the prevalence of good cord care practice is high, there is still a use of potentially harmful substances for cord care and still many neonates are at risk of developing Omphalitis and neonatal sepsis.
Acronyms and abbreviations
ANC: Antenatal Care
AOR: Adjusted Odds Ratio
CSA: Central Statics Agency
COR: Crude odds ratio
EBF: Exclusive Breast Feeding
EDHS: Ethiopian Demographic and Health Survey
ETB: Ethiopian Birr
ENC: Essential Newborn Care
HI: Health Institution
LMICs- Low and Middle Income Countries
MDG: Millennium Development Goal
SPSS: Statistical Package for Social Science
SDG: Sustainable development goals
WHO: World Health Organization
Acknowledgment
We would like to thank Mekelle University, College of Health sciences, Tigray Region Health Bureau, Mekelle city health office, study participants, and data collectors for their contribution in the success of our work
Funding Statement
The research for this project is unfunded. The authors paid for all expenses associated with gathering and analyzing the data.
Data availability
The data sets during and/or analyzed during the current study available from the corresponding author on reasonable request
Authors' contributions
SA: conceived and designed the study, analyzed the data and wrote the manuscript. GK, GA, AB, TA, GG, BH, AG, involved in data analysis, drafting of the manuscript and advising the whole research paper and also were involved in the interpretation of the data and contributed to manuscript preparation. Similarly, all authors have read and approved the final version of the manuscript.
Ethical approval and consent to participate
Ethical clearance was obtained from the ethical review board of Mekelle University College of health science to Mekelle city administration health office, then to each elected sub-cities; Informed, written and signed consent was obtained from each health office coordinator of the sub-cities. Informed consent was obtained from each participant after explaining the purpose and benefits of the study. Participants were informed about the minimal risk that it had taking part in the study, their volunteerism and the right to leave the interview at any time they want. Confidentiality of the study participants’ information was also ensured by coding the questionnaire.
Competing Interests
The author(s) of this manuscript have not disclosed any financial conflicts of interest with this work, nor have they indicated any non-financial conflicts of interest with this work, such as political, personal, religious, ideological, academic, commercial, or any other conflicts.
Conclusion
Even though the prevalence of good cord care practice is high, there is still a use of potentially harmful substances for cord care and still many neonates are at risk of developing Omphalitis and neonatal sepsis.
Acronyms and abbreviations
ANC: Antenatal Care
AOR: Adjusted Odds Ratio
CSA: Central Statics Agency
COR: Crude odds ratio
EBF: Exclusive Breast Feeding
EDHS: Ethiopian Demographic and Health Survey
ETB: Ethiopian Birr
ENC: Essential Newborn Care
HI: Health Institution
LMICs- Low and Middle Income Countries
MDG: Millennium Development Goal
SPSS: Statistical Package for Social Science
SDG: Sustainable development goals
WHO: World Health Organization
Acknowledgment
We would like to thank Mekelle University, College of Health sciences, Tigray Region Health Bureau, Mekelle city health office, study participants, and data collectors for their contribution in the success of our work
Funding Statement
The research for this project is unfunded. The authors paid for all expenses associated with gathering and analyzing the data.
Data availability
The data sets during and/or analyzed during the current study available from the corresponding author on reasonable request
Authors' contributions
SA: conceived and designed the study, analyzed the data and wrote the manuscript. GK, GA, AB, TA, GG, BH, AG, involved in data analysis, drafting of the manuscript and advising the whole research paper and also were involved in the interpretation of the data and contributed to manuscript preparation. Similarly, all authors have read and approved the final version of the manuscript.
Ethical approval and consent to participate
Ethical clearance was obtained from the ethical review board of Mekelle University College of health science to Mekelle city administration health office, then to each elected sub-cities; Informed, written and signed consent was obtained from each health office coordinator of the sub-cities. Informed consent was obtained from each participant after explaining the purpose and benefits of the study. Participants were informed about the minimal risk that it had taking part in the study, their volunteerism and the right to leave the interview at any time they want. Confidentiality of the study participants’ information was also ensured by coding the questionnaire.
Competing Interests
The author(s) of this manuscript have not disclosed any financial conflicts of interest with this work, nor have they indicated any non-financial conflicts of interest with this work, such as political, personal, religious, ideological, academic, commercial, or any other conflicts.
References
-
Afolaranmi TO. Cord Care Practices: A Perspective of Contemporary African Setting. Front Public Heal |. 2018;6(January):1–2.
Publisher | Google Scholor -
Gallina L, De Tina AL, Basso T, Brusaferro S, Quattrin R. Umbilical cord care after the first day from birth: a case control study in a Northeastern Italian Hospital. Pediatr Neonatal Nurs Open J. 2016; 3(1): 4-9.
Publisher | Google Scholor -
WHO Reproductive Health (Technical Support) Maternal and Newborn Health / Safe Motherhood Care of the Umbilical Cord: A review of the evidence, 1998 :(4) 7-10
Publisher | Google Scholor -
Blessing I. Abhulimhen‑Iyoha, Michael O. Ibadin, Cord care education and its content given to mothers at antenatal clinics in various health facilities in Edo state, Nigeria, Sahel Medical Journal / July-September 2015 / Vol 18 | 1-3
Publisher | Google Scholor -
B., Malik J.S., Jindal H., Sahoo S. and Sangwan K, A study to assess cord care practices among mothers of new borns in urban areas of Rohtak Haryana , International Journal of Basic and Applied Medical Sciences,2015(5),2-4
--> -
Lawrence, Arunibebi Lamawal1, Jimmy, Jessica Agada1, Aluye-Benibo, Igbans, Umbilical Cord Care Practices by Traditional Birth Attendants in Yenagoa, Nigeria Journal of Nursing and Health Science, Mar.-Apr. 2015,(4) 1-2
Publisher | Google Scholor -
OsuorahDonatus I Chidiebere, EkwochiUchenna, OnahStanley,and E. Ebruke Bernard, , Umbilical Cord Care Practices and Incidence of Febrile Illnesses in the First Month of Life among Newborns- A Population Based Study, British Journal of Medicine & Medical Research 2014, (5) 2-5.
Publisher | Google Scholor -
Amare Y. Umbilical cord care in Ethiopia and implications for behavioral change: BMC International Health and Human Rights. 2014; 14(1):1–8.
Publisher | Google Scholor -
Sartaj Ahmad, KapilGoel, GaganAgarwal, ParulGoel, Vijay Kumar and AshishPrakash, , Assessment of the Newborn Care Practices in Home Deliveries among Urban Slums of Meerut, UP India,Journal of Community Medicine & Health Education an open access journal, 2012 (2)8, 1-3
Publisher | Google Scholor -
Gallina L, De Tina AL, Basso T, Brusaferro S, Quattrin R. Umbilical cord care after the first day from birth: a case control study in a Northeastern Italian Hospital. Pediatr Neonatal Nurs Open J. 2016; 3(1): 4-9.
Publisher | Google Scholor -
Rachel Musoke, Fred Were, E. Obimbo, Knowledge, attitudes and practices of mothers and knowledge of health workers regarding care of the newborn umbilical cord, East African medical journal • September 1999, 2-6
Publisher | Google Scholor -
Darling B, Wankhede RS, Benjamin BA. A descriptive study on newborn care among postnatal mothers inselected maternity centersin madurai , Tamilnadu . nternational J Allied Med Sci Clin Res I. 2014;2(2):119–24.
--> -
Agossou, J., Hounnou-d’Almeïda, M., Adédémy, J.D., Noudamadjo, A., N’gobi, D.Y.G. and Ayivi, B. Newborn Umbilical
Publisher | Google Scholor -
Kolola T, Ekubay M, Tesfa E, Morka W. Determinants of Neonatal Mortality in North Shoa Zone , Amhara Regional State , Ethiopia. PLoSONE 2016;1–11
Publisher | Google Scholor -
WHO, Countrycooperation strategy, south Sudan May 2018.3-4 (WHO/CCU/18.02 South Sudan )
--> -
UNICEF,Maternal and Newborn Health Disparities, in Ethiopia. 2011.
--> -
the United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) UNICEF, WHO, United Nations Population Division and the World Bank).) 2018
--> -
TensouB, Telake1 Daniel S, And Tedbabe Degefie, BekeleAbeba. Neonatal mortality in Ethiopia_ trends and determinants _ BMC Public Health . 2013;13:483
--> -
Peter Waiswa, Stefan Peterson, GoranTomson, George W Pariyo1 Poor newborn care practices - a population based survey in eastern Uganda, BMC Pregnancy and Childbirth 2010, 10:4-6
--> -
Mersha A, Assefa N, Teji K, Shibiru S, Darghawth R, Bante A. Essential newborn care practice and its predictors among mother who delivered within the past six months in Chencha District ,. OPEN ACCES. 2018;1–17
Publisher | Google Scholor -
Berhe M, Medhaniye AA, Kahsay G, Birhane E, Abay, Essential neonatal careutilization and associated factors among mothers in public health facilities of Aksum Town, North Ethiopia, PLoS ONE ,2016. 12(4): 5-9
--> -
GerezgiherBuruhAbera, HailemariamBerhe and Haftom G/ Hiwet, assessment of newborn care practices of mothers in mereblekeeuropean journal of pharmaceutical and medical research, 2016;3(9):6–12
--> -
Sinha RC, Lal BS, Regmi B, Pant B. Newborn Care Practices among Mothers in Rautahat District , Nepal. Nepal Public Heal Assoc. 2013;5(1):19–24.
--> -
Opara PI, Jaja T, Dotimi DA, Alex-hart BA. Newborn Cord Care Practices amongst Mothers in Yenagoa Local Government Area , Bayelsa State , Nigeria. Int J Clin Med. 2012;2012(January):22–7
Publisher | Google Scholor -
Patricia S. Coffey and Siobhan, Umbilical cord-care practices in low- and middle income countries : a systematic review. BMC Pregnancy and Childbirth (2017) 17;4–12
Publisher | Google Scholor -
Saaka M, Ali F, Vuu F. Prevalence and determinants of essential newborn care practices in the Lawra District of Ghana. BMC Pediatrics (2018) 18 2018;1–12.
Publisher | Google Scholor -
chaudhary j, dhungana gp, ghimire h. factors affecting newborn care practices among tharu mothers in selected village development committees of chitwan district. Journal of chitwan medical college 2013,. 2013;(3):4–9
Publisher | Google Scholor